
Rehabilitation Case Study
Mr. B admitted to Cedar View Rehabilitation and Healthcare Center on May 06, 2022 under the care of Dr. Janarthanan Someswarananthan. During the course of the stay, Occupational Therapy, and Physical Therapy were initiated to efficiently and effectively identify his unique needs and tailor specialized treatment plans to successfully transition to the next level of care.
On admission, he was noted to require minimal assistance with bathing and lower body dressing, contact guard assistance with ambulation, standby assistance with hygiene tasks, toileting, bathing and transfers and supervision with upper body dressing. Decreased balance and deconditioning also increased his risk for falling. he has been working with the interdisciplinary team and participating in care plan meetings and therapy throughout his stay. His participation was limited in the beginning due to weakness and overall deconditioning, but as he improved and increased his strength, he was able to increase his participation in higher level functional activities.
The therapy team provided skilled interventions to address his adaptation, compensation, and restoration potential and coordinated with the interdisciplinary team to ensure appropriate clinical care areas were addressed. On May 18, 2022, he successfully discharged home being able to complete bathing, hygiene tasks, dressing and toileting independently and bed mobility, transfers and ambulation with modified independence. Great work Mr. B!
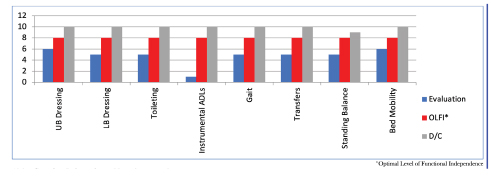
Overall Composite Score Outcomes
Rehabilitation outcomes are assessed on a 10-point rating scale. 10 is the most independent level of ability, and 1 is the most dependent level of ability. A score of 0 may represent an inability to perform the task. The Model 10 Composite Score represents his overall outcomes.
Rehabilitation Length of Stay: 13 Days
Functional Outcome Level Upon Admission: 5.5
Functional Outcome Level Upon Discharge: 9.6
Rehabilitation Case Study
Ms. L admitted to Cedar View Rehabilitation and Healthcare Center on June 14, 2022 under the care of Dr. Janarthanan Someswarananthan. During the course of the stay, Occupational Therapy, and Physical Therapy were initiated to efficiently and effectively identify her unique needs and tailor specialized treatment plans to successfully transition to the next level of care.
On admission, she was noted to require minimal assistance with lower body dressing, contact guard assistance with bathing, toileting, ambulation and transfers and setup assistance with upper body dressing. Decreased balance and activity tolerance also increased her risk for falling. She has been working with the interdisciplinary team and participating in care plan meetings and therapy throughout her stay. Her participation was limited in the beginning of her stay due to weakness and overall deconditioning, but as she improved and increased her strength, she was able to increase her participation in higher level functional activities.
The therapy team provided skilled interventions to address her adaptation, compensation, and restoration potential and coordinated with the interdisciplinary team to ensure appropriate clinical care areas were addressed. On June 25, 2022, she successfully discharged home being able to complete upper body dressing independently and bathing, lower body dressing, toileting, ambulation and transfers with modified independence. Great work Ms. L!
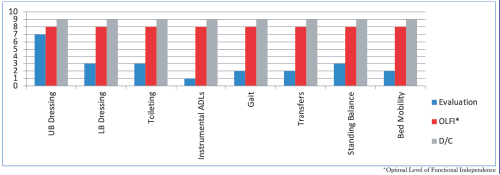
Overall Composite Score Outcomes
Rehabilitation outcomes are assessed on a 10-point rating scale. 10 is the most independent level of ability, and 1 is the most dependent level of ability. A score of 0 may represent an inability to perform the task. The Model 10 Composite Score represents his overall outcomes.
Rehabilitation Length of Stay: 12 Days
Functional Outcome Level Upon Admission: 5.3
Functional Outcome Level Upon Discharge: 9.2
Rehabilitation Case Study
Ms. T admitted to Cedar View Rehabilitation and Healthcare Center on August 17, 2022 under the care of Dr. Janarthanan Someswarananthan. During the course of the stay, Occupational Therapy, and Physical Therapy were initiated to efficiently and effectively identify her unique needs and tailor specialized treatment plans to successfully transition to the next level of care.
On admission, she was noted to require minimal assistance with toileting, contact guard assistance with bathing and hygiene tasks and standby assistance with upper body dressing, bed mobility, ambulation and transfers. Decreased balance and activity tolerance also increased her risk for falling. She has been working with the interdisciplinary team and participating in care plan meetings and therapy throughout her stay. Her participation was limited in the beginning of her stay due to weakness and overall deconditioning, but as she improved and increased her strength, she was able to increase her participation in higher level functional activities.
The therapy team provided skilled interventions to address her adaptation, compensation, and restoration potential and coordinated with the interdisciplinary team to ensure appropriate clinical care areas were addressed. On August 25, 2022, she successfully discharged home being able to complete hygiene tasks independently and bathing, toileting, upper body dressing, bed mobility, ambulation and transfers with modified independence. Great work Ms. T!
Overall Composite Score Outcomes
Rehabilitation outcomes are assessed on a 10-point rating scale. 10 is the most independent level of ability, and 1 is the most dependent level of ability. A score of 0 may represent an inability to perform the task. The Model 10 Composite Score represents his overall outcomes.
Rehabilitation Length of Stay: 9 Days
Functional Outcome Level Upon Admission: 5.4
Functional Outcome Level Upon Discharge: 9.1
Case Study
Admitting Diagnosis: Pneumonia
Specialty Program: Pulmonary
Discharge Location: Home
A 55-year-old gentleman was admitted to Cedar View Rehabilitation and Healthcare Center from Holy Family Hospital on October 30, 2020 for skilled nursing and therapy services to safely return home. Upon admission, Mr. H. was evaluated by and participated in skilled occupational and physical therapy where he was noted to require contact guard assistance for most self-care tasks, to transfer and ambulate 50 feet, standby assistance to perform bed mobility and was noted to have decreased balance and activity tolerance increasing his risk for falls. As he progressed with his therapy goals, he was able to participate in higher level functional activities such as stair training and car transfers while maintaining his safety. Upon discharge, Mr. H. was able to perform all self-care tasks, bed mobility, transfer, ambulate 1000 feet with no adaptive device and ascend and descend 12 stairs independently while maintaining his low fall risk tasks. He made great gains toward his therapy and was able to return home with home care services. Great work Mr. H.!
10.0 – Complete Independent – No assist, no equipment
9.0 – Modified Independent – No Assist, but equipment or extra time
8.0 – S/u – No physical assist other than set-up; supervision for safety/technique; and/or single cue to initiate
7.0 – Supervision-No physical assist; supervision for safety/technique; and/or single cue to initiate
6.0 – SBA-Pt. performs task with close supervision and or visual/verbal cues for task completion
5.0 – CGA – Contact Guard Assist
4.0 – Min – Occasional assist (25% or less time or effort to complete)
3.0 – Mod – Frequent assist (40-50% of the time or effort involved to complete task
2.0 – Max – Constant assist (75-90% of the time or effort involved to complete task
1.0 – CD – Complete Dependence: No contribution from pt; task done by others or not assessed
Case Study
Admitting Diagnosis: Spinal Fusion, Lumbar Region
Discharge Location: Home
A 67-year-old female was admitted to Cedar View Rehabilitation and Healthcare Center from Lawrence General Hospital for skilled nursing and therapy services to safely return home. Upon admission, Mrs. T. was evaluated by and participated in skilled occupational and physical therapy where she was note to require moderate/maximum assistance for most selfcare tasks, bed mobility, transfers and gait and was noted to have decreased balance and activity tolerance increasing her risk for falls. As she progressed with her therapy goals, she was able to participate in higher level functional activities such as balance training, stair training and car transfers while maintaining her safety. Upon discharge, Mrs. T. was able to perform all selfcare tasks, bed mobility, was able to transfer and ambulate 100 feet with modified independence and was able to ascend and descend 4 stairs with supervision. She was a low fall risk and had decreased pain. She made great gains toward her therapy goals and was able to return home with strong family support and home health services. Great work Mrs. T.!
10.0 – Complete Independent – No assist, no equipment
9.0 – Modified Independent – No Assist, but equipment or extra time
8.0 – S/u – No physical assist other than set-up; supervision for safety/technique; and/or single cue to initiate
7.0 – Supervision-No physical assist; supervision for safety/technique; and/or single cue to initiate
6.0 – SBA-Pt. performs task with close supervision and or visual/verbal cues for task completion
5.0 – CGA – Contact Guard Assist
4.0 – Min – Occasional assist (25% or less time or effort to complete)
3.0 – Mod – Frequent assist (40-50% of the time or effort involved to complete task
2.0 – Max – Constant assist (75-90% of the time or effort involved to complete task
1.0 – CD – Complete Dependence: No contribution from pt; task done by others or not assessed